CFTI Therapy Models
What is EMDR?
The mind can often heal itself naturally, in the same way as the body does. Much of this natural coping mechanism occurs during sleep, particularly during rapid eye movement (REM) sleep. Francine Shapiro developed Eye Movement Desensitization and Reprocessing (EMDR) in 1987, utilizing this natural process in order to successfully treat Post-traumatic Stress Disorder (PTSD). Since then, EMDR has been used to effectively treat a wide range of mental health problems.
What happens when you are traumatized?
Most of the time, your body routinely manages new information and experiences without you being aware of it. However, when something out of the ordinary occurs and you are traumatized by an overwhelming event (e.g. a car accident) or by being repeatedly subjected to distress (e.g. childhood neglect), your natural coping mechanism can become overloaded. This overloading can result in disturbing experiences remaining frozen in your brain or being “unprocessed”. Such unprocessed memories and feelings are stored in the limbic system of your brain in a “raw” and emotional form, rather than in a verbal “story” mode. This limbic system maintains traumatic memories in an isolated memory network that is associated with emotions and physical sensations, which are disconnected from the brain’s cortex where we use language to store memories. The limbic system’s traumatic memories can be continually triggered when you experience events similar to the difficult experiences you have been through. Often the memory itself is long forgotten, but the painful feelings such as anxiety, panic, anger or despair are continually triggered in the present. Your ability to live in the present and learn from new experiences can therefore become inhibited. EMDR helps create the connections between your brain’s memory networks, enabling your brain to process the traumatic memory in a very natural way.
What is an EMDR session like?
EMDR utilizes the natural healing ability of your body. After a thorough assessment and development of a treatment plan, you will be asked specific questions about a particular disturbing memory. Eye movements, similar to those during REM sleep, will be recreated simply by asking you to watch the therapist’s finger moving backwards and forwards across your visual field. Sometimes, a bar of moving lights or headphones or Tapping is used instead. The eye movements will last for a short while and then stop. You will then be asked to report back on the experiences you have had during each of these sets of eye movements. Experiences during a session may include changes in thoughts, images and feelings.
With repeated sets of eye movements, the memory tends to change in such a way that it loses its painful intensity and simply becomes a neutral memory of an event in the past. Other associated memories may also heal at the same time. This linking of related memories can lead to a dramatic and rapid improvement in many aspects of your life.
What can EMDR be used for?
In addition to its use for the treatment of Post-Traumatic Stress Disorder, EMDR has been successfully used to treat:
anxiety and panic attacks depression, PTSD anger phobias
sleep problems
grief and loss addictions pain, including phantom limb pain performance anxiety feelings of worthlessness/low self-esteem
Before and after EMDR brain scans.
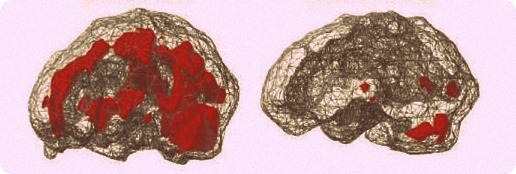
Left photo shows woman with Post Traumatic Stress Disorder. Right photo shows same woman after four ninety minute EMDR sessions. The brightened areas indicate over-activity in the brain. Photo by Dr. Daniel Amen
Can anyone benefit from EMDR?
EMDR can accelerate therapy by resolving the impact of your past traumas and allowing you to live more fully in the present. It is not, however, appropriate for everyone. The process is rapid, and any disturbing experiences, if they occur at all, last for a comparatively short period of time. Nevertheless, you need to be aware of, and willing to experience, the strong feelings and disturbing thoughts that sometimes occur during sessions.
How long does treatment take?
EMDR can be brief focused treatment or part of a longer psychotherapy treatment plan. EMDR can be easily integrated with other approaches in which your therapist might be trained, such as Psychodynamic psychotherapy, Dialectical Behavior Therapy, or Cognitive Behavior Therapy. For best effects, EMDR sessions during the actual reprocessing phases of treatment usually last from 60 to 90 minutes. Positive effects have been seen after one session of EMDR.
Will I will remain in control and empowered?
During EMDR treatment, you will remain in control, fully alert and wide-awake. This is not a form of hypnosis and you can stop the process at any time. Throughout the session, the therapist will support and facilitate your own self-healing and intervene as little as possible. Reprocessing is usually experienced as something that happens spontaneously, and new connections and insights are felt to arise quite naturally from within. As a result, most people experience EMDR as being a natural and very empowering therapy.
What evidence is there that EMDR is a successful treatment?
EMDR is an innovative clinical treatment that has successfully helped over a million individuals. The validity and reliability of EMDR has been established by rigorous research. There are now over nineteen controlled studies into EMDR, making it the most thoroughly researched method used in the treatment of trauma, and The American Psychiatric Association, American Psychological Association, Department of Defense, Veteran’s Administration, insurance companies, and the International Society for Traumatic Stress Studies recognize EMDR as an effective treatment for PTSD. For further information about EMDR, point your Internet browser to www.emdria.org or www.emdr.com.